breast cancer
Enough about television and my damn cold that just won't go away completely (down to just a cough now, thanks for asking!), now it's back to something more serious. Breast cancer. In case you've not been here before, research on breast cancer is what I do for a living. I use molecular biological techniques, particularly DNA microarrays, to determine what effects, if any, drugs have on the proliferation of breast cancer cells both in vivo and in vitro.
 2-methoxyestradiol (2ME) is my main focus these days and it's in the body of almost every woman already. That's because it's a natural breakdown product of estrogen. Using 2ME clinically requires higher doses than normally appears in the body and its use is still experimental with clinical trials taking place in several places in the US.
2-methoxyestradiol (2ME) is my main focus these days and it's in the body of almost every woman already. That's because it's a natural breakdown product of estrogen. Using 2ME clinically requires higher doses than normally appears in the body and its use is still experimental with clinical trials taking place in several places in the US.
But that's all beside the point since my topic for today is the difference in cancer outcome across ethnic groups. I was just giving some background up there.
African American women die from cancer at much higher rates than women of other ethnic groups. For a long time it's been assumed that the poor outcome for African American women resulted from delayed treatment due to poorer medical care and the patient not detecting the cancer at as early a stage (as most people know these days, early detection of cancer is the biggest factor in survival rate). These assumptions have been revised lately. While there's no denying the fact that race and income level do have effects on patient care and outcome, there's more to the story regarding African American women and breast cancer.
Breast cancer is not a monolithic disease. There's different types of breast cancer and we distinguish them by the surface markers that are on the cells and how the cells react to estrogen. Two of the major types of tumor are basal and luminal. Basal cell tumors are ER- (negative for estrogen receptors) and HER2 negative (the human epidermal growth factor receptor-2 is not present on the cells). Currently we don't have drugs that specifically target the estrogen or HER2 pathways so basal cell tumors don't have as many treatment options. As a result basal tumors are much more deadly than luminal tumors since only chemotherapy is available as a treatment. Unfortunately African American women are much more likely to have basal tumors than luminal and women of European ancestry tend towards luminal tumors. While there are drugs in clinical trials for basal-like cancer cells, nothing is on the market yet.
Typing tumors like this is a very recent development. The recent use of DNA microarrays has dramatically increased our knowledge of how cells react genetically to cancer and how different genetic profiles are more at risk for certain types of cancer.
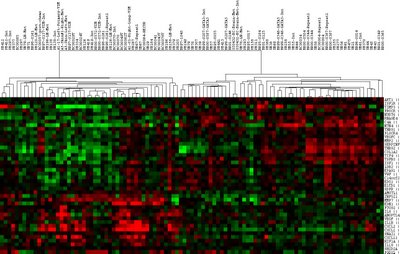 At left is a plot of some data we have of luminal versus basal cell types. You can see that the red (up regulated genes) and green (down regulated genes) tend to cluster when using a grouping of angiogenesis genes for the microarrays.
At left is a plot of some data we have of luminal versus basal cell types. You can see that the red (up regulated genes) and green (down regulated genes) tend to cluster when using a grouping of angiogenesis genes for the microarrays.
Angiogenesis is the process of making new blood vessels and a process that cancer tumors have to be able to initiate in order to grow in size. Selectively preventing angiogenesis is one strategy for controlling cancer.
The word selective is quite important since there's all sorts of tissues in the body that need new blood vessels that we don't want to harm. Medicine sure is complicated.
 2-methoxyestradiol (2ME) is my main focus these days and it's in the body of almost every woman already. That's because it's a natural breakdown product of estrogen. Using 2ME clinically requires higher doses than normally appears in the body and its use is still experimental with clinical trials taking place in several places in the US.
2-methoxyestradiol (2ME) is my main focus these days and it's in the body of almost every woman already. That's because it's a natural breakdown product of estrogen. Using 2ME clinically requires higher doses than normally appears in the body and its use is still experimental with clinical trials taking place in several places in the US.But that's all beside the point since my topic for today is the difference in cancer outcome across ethnic groups. I was just giving some background up there.
African American women die from cancer at much higher rates than women of other ethnic groups. For a long time it's been assumed that the poor outcome for African American women resulted from delayed treatment due to poorer medical care and the patient not detecting the cancer at as early a stage (as most people know these days, early detection of cancer is the biggest factor in survival rate). These assumptions have been revised lately. While there's no denying the fact that race and income level do have effects on patient care and outcome, there's more to the story regarding African American women and breast cancer.
Breast cancer is not a monolithic disease. There's different types of breast cancer and we distinguish them by the surface markers that are on the cells and how the cells react to estrogen. Two of the major types of tumor are basal and luminal. Basal cell tumors are ER- (negative for estrogen receptors) and HER2 negative (the human epidermal growth factor receptor-2 is not present on the cells). Currently we don't have drugs that specifically target the estrogen or HER2 pathways so basal cell tumors don't have as many treatment options. As a result basal tumors are much more deadly than luminal tumors since only chemotherapy is available as a treatment. Unfortunately African American women are much more likely to have basal tumors than luminal and women of European ancestry tend towards luminal tumors. While there are drugs in clinical trials for basal-like cancer cells, nothing is on the market yet.
Typing tumors like this is a very recent development. The recent use of DNA microarrays has dramatically increased our knowledge of how cells react genetically to cancer and how different genetic profiles are more at risk for certain types of cancer.
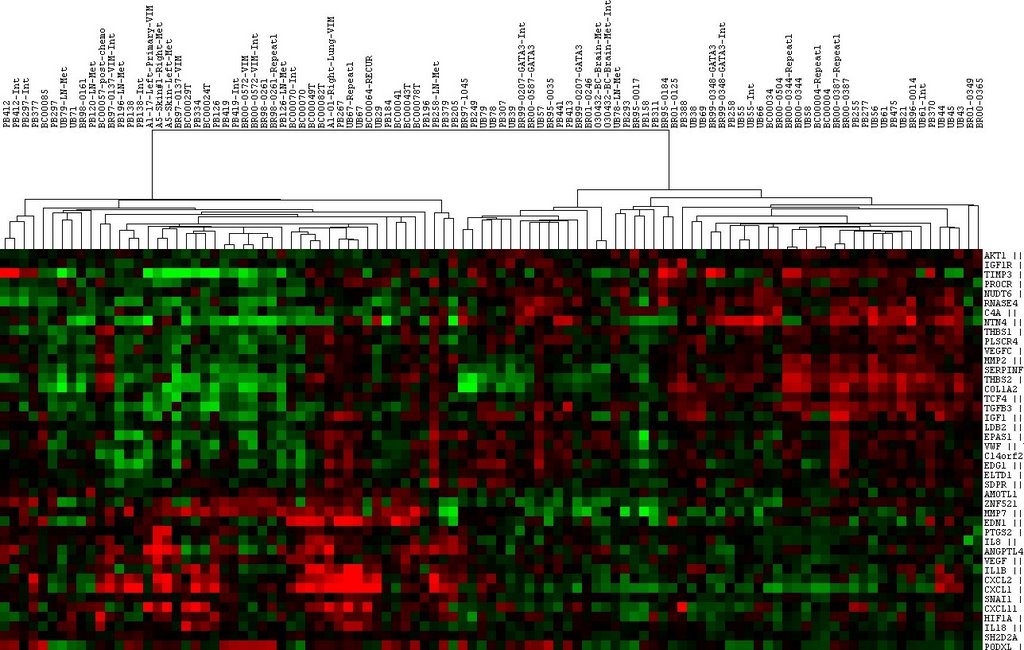 At left is a plot of some data we have of luminal versus basal cell types. You can see that the red (up regulated genes) and green (down regulated genes) tend to cluster when using a grouping of angiogenesis genes for the microarrays.
At left is a plot of some data we have of luminal versus basal cell types. You can see that the red (up regulated genes) and green (down regulated genes) tend to cluster when using a grouping of angiogenesis genes for the microarrays.Angiogenesis is the process of making new blood vessels and a process that cancer tumors have to be able to initiate in order to grow in size. Selectively preventing angiogenesis is one strategy for controlling cancer.
The word selective is quite important since there's all sorts of tissues in the body that need new blood vessels that we don't want to harm. Medicine sure is complicated.



Comments
Thanks for stopping by my blog and making me feel better.
We seem to understand a lot but it is still so sad that many of us know someone directly affected.
Its the birthday today of the son of a friend of mine. My friend was briefly in tears today thinking about handing over the birthday card from his recently departed wife who died from cancer.
Becky wrote cards to their son's 21st birthdays.
Michele sent me today.
Hope you are feeling better!
Such an informative post Dave, keep up the great research :o)
I can't help but read your entry and think that the future is bright, and that there may yet come a day when we can beat this thing. We're in good research hands, thanks to you.
Has any of your research looked at the difference in the types of breast cancer that strikes pre-menopausal women vs. that of post-menopausal women. Basal vs. luminal. And I assume this is pertaining to infiltrating ductal carcinoma since lobular carcinoma and colloid (mucinous) carcinoma have much different clinical behaviors.
It's has always seemed to me from seeing clinical reports and from experience in our labs, that invasive ductal carcinoma is most devastating in young women who often have widespread node mets, huge tumors, negative receptors and such.
My ex-brother-in-law is an engineer for Bell Helicopter. He went back to get his PhD and decided to work with a physician at Southwestern Med School in Dallas. His work was developing a mathematical model to help physicians predict outcome from various clinical factors.
You are right, medicine is very, very complicated.
my mother is a breast cancer survivor. happily it was found INCREDIBLY early. the docs moved quickly and she's 5 years out. she is going tomorrow, in fact, to talk w/her oncologist in town (when she had it, she was in columbus, oh, now she's in sparks, nv). he wants her to take a new drug now that she's done w/the tomoxifin.
she and i walked in the Avon 2 day walk in SF in 2004. it was emotional doing it with her. i need to find a doc and start getting mamograms - but up until last week i was still nursing.
anyway, i just wanted to say thank you.